
Draft Winter (21/22), Respiratory Infections in Health and Care Settings Infection Prevention and Control (IPC) Addendum
Draft 5.1 Introduction
This guidance has been developed during the ongoing COVID-19 pandemic recognising the likelihood of a surge in other respiratory viruses in addition to COVID-19 over the winter season of 2021/22 and supersedes the 3 COVID-19 addenda (Acute, Care home and Community health and care settings) first published in October 2020. This guidance is aligned with the UK Infection Prevention and Control for Seasonal Respiratory Infections in Health and Care settings including SARS-CoV-2 for Autumn Winter 2021/2022. High consequence infection diseases (HCIDs) transmitted by the airborne route such as emerging pandemic influenza or other novel respiratory viruses are out of scope for this guidance.
Key changes as we move from the COVID-19 addenda to Winter (21/22), Respiratory Infections in Health and Care Settings Infection Prevention and Control (IPC) Addendum are;
- Removal of the 3 distinct COVID-19 care pathways (high/red, medium/amber and low/green) to respiratory and non–respiratory pathways
- A return to Standard Infection Control Precautions (SICPs) and Transmission Based Precautions (TBPs) as per National Infection Prevention and Control Manual (NIPCM) and the Care Home Infection Prevention and Control Manual (CHIPCM)
- An algorithm to support placement of service users within health and care settings
- Respiratory screening questions to include COVID-19 AND other respiratory pathogens
- Ongoing Rapid testing for COVID-19 AND to now include other respiratory pathogens in some settings
It should be noted that the principles of applying TBPs for service users presenting with a suspected/confirmed respiratory virus apply at all times throughout the year however the purpose of this guidance is to support health and care settings when cases of respiratory viruses/infections increase impacting on flow and service delivery.
NHS Scotland boards are preparing for an increase in service demand as a result of respiratory virus this winter season (21/22) and this guidance should be implemented to minimise risk and harm to staff, service users and visitors during this period of increased admissions and whilst the COVID-19 pandemic continues. It is intended that this guidance will be reviewed regularly and adapted for use routinely on an annual basis.
IPC measures required for COVID-19 are incorporated within this guidance and IPC principles are applied consistently across all respiratory pathogens wherever possible. Some pandemic measures specific to COVID-19 remain at this time and these will be highlighted within this guidance.
Although many of the COVID-19 pandemic measures within the general community are relaxing, there remains a very real risk within healthcare settings of COVID-19 transmission and transmission of other respiratory pathogens e.g Influenza, Respiratory Syncytial Virus (RSV), Rhinovirus. This is due to compounding factors such as vulnerability of the service users, the communal nature of many of the care facilities and within primary and secondary care settings, the very nature of the service provided in treating respiratory infections which facilitates the presence of high numbers of symptomatic individuals in the setting.
The term ‘service users’ will be used in generic sections to describe patients, residents and individuals.
This guidance is intended for use by all those involved in health and care provision and applies to the following settings;
- Secondary care (Acute) including paediatrics & mental health
- Primary care
- Mental Health services
- Care homes
- GP practices/health centres
- Dental settings (across all sectors including secondary care)
- Hospice settings
- Community Optometry
- Community Pharmacy
- Specialist palliative care in-patients units/hospices
- Health and social care services provided in peoples own homes
- Community based health and care settings
- Care at home
- Supported accommodation settings
- Rehabilitation services
- Residential children's homes
- Stand-alone residential respite for adults (settings not registered as a care home)
- Stand-alone residential respite/short break services for children
- Sheltered housing
- Health centres within Prison and detention settings
- Scottish Ambulance service (SAS) – NB: SAS also have specific setting guidance
This guidance is generic to all the settings described above however, where specific sector guidance exists it will be highlighted as follows;
Guidance specific to Secondary care settings or particular services within secondary care will be highlighted in blue.
Guidance specific to Primary care and Community Health and Social Care settings or particular services within primary care or health and social care will be highlighted in green.
Guidance specific to Care home settings or particular services within the care home settings will be highlighted in pink.
Guidance specific to Dental settings or particular services within dental settings will be highlighted in lilac. (Dental services operating in secondary care settings may also choose to refer to guidance specific to secondary care)
Draft 5.2 Organisational Preparedness
All health and care settings must make efforts to prepare and plan for an increase in cases of respiratory viruses and as such the management of respiratory viruses in advance of the respiratory season. IPC should form part of winter planning for NHS boards and other care providers. The impact of the respiratory season on individual settings will vary depending on;
- The throughput of service users within the setting
- The vulnerability of service users within the setting in terms of potential exposure to respiratory viruses and risk of severe disease should they acquire a respiratory virus
- The ability to isolate service users within the setting
- Access to testing for respiratory pathogens
Health and care settings and in some cases, individual departments e.g. emergency departments, critical care units are encouraged to develop a respiratory plan applicable for their area. Examples of considerations within the respiratory plan may include;
- the process for service user respiratory screening,
- placement and segregation of service users with respiratory symptoms or a confirmed respiratory virus/infection
- testing arrangements,
- staff resource, allocation (inclusive of plans for increased staff absence)
- the expansion of respiratory support and Intensive Care Units (ICUs) should this be required
Draft 5.3 Hierarchy of controls
5.3.1 Ventilation in health and care settings
5.3.2 Mechanically ventilated areas
5.3.3 Naturally ventilated areas (no mechanical ventilation)
5.3.5 Bed and treatment chair spacing
Controlling exposures to occupational hazards, including the risk of infection, is the fundamental method of protecting users of the health and care facilities. Figure 1 is a graphic specifying the general principles of prevention legislated in the Management of Health and Safety at Work Regulations 1999, Regulation 4, Schedule 1. It details the most to the least effective hierarchy of controls and can be used to help implement effective controls in preventing the spread of respiratory viruses within health and care settings. The hierarchy of controls will help protect all users of the health and care facility and not just staff. NHS Boards/care organisations and staff should first employ the most effective method of control which inherently results in safer control systems. Where that is not possible, all others must be considered in sequence. Personal protective equipment (PPE) is the last in the hierarchy of controls and may be the only mitigating control when caring for a service user with a pathogen spread by the airborne route.
Figure 1: Hierarchy of controls diagram
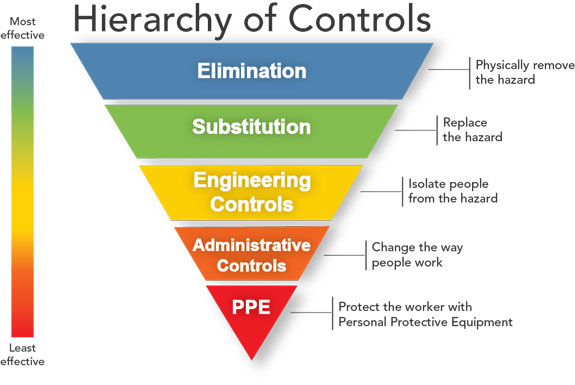
Centers for disease control and prevention. The National Institute for Occupational Safety and Health. Hierarchy of Controls. 2015.
Examples of ways in which the hierarchy of controls can be applied in health and care settings is as follows (note these are example; not all will apply in every health and care setting and generally apply to both the respiratory and non-respiratory pathways unless otherwise stated);
Table 1: Hierarchy of controls examples in practice
Hierarchy of controls |
Example in practice and resources |
|---|---|
Elimination
|
|
Substitution |
|
Engineering controls
|
|
|
Administration controls |
|
|
Personal Protective Equipment (PPE) |
|
Some health and care settings and service user groups present a greater risk for the transmission of respiratory viruses. Health and care settings must seek to identify and prepare the most suitable clinical/care area for planned placement of service users requiring care on the respiratory pathway.
 Secondary Care settings
Secondary Care settings
Risk assessing placement of the inpatient respiratory pathway
Prior to determining areas for planned placement of the respiratory pathway, the NHS Board/Organisation must ensure a full structured risk assessment of the proposed area is carried out, led by operational and clinical management and involving health and safety teams, Estates and Facilities representatives, Occupational Health Services (OHS), Infection Prevention & Control Team (IPCT) and the clinical team. This should be undertaken using the hierarchy of controls and recognise that there is lowest risk where elimination can be achieved and highest risk where PPE is the only control in place. Risk assessments should be periodically reviewed as determined by the NHS Board/care organisation to ensure no change to the level of risk. A Risk Assessment algorithm was developed for COVID-19 patient placement but can be applied to the respiratory pathway. The algorithm aims to help support the risk assessment process and should take account of the following;
-
-
- Does the room capacity allow for all bed/treatment chairs to meet 2m physical distancing requirements as a minimum?
- Is the area mechanically ventilated and meet a minimum of 6 air changes per hour (ACH)?
-
If the risk assessment concludes that an unacceptable risk of transmission remains within the environment after rigorous application of the hierarchy of controls (e.g. inadequate spacing to allow for required bed/treatment chair occupancy AND ventilation of less than 6ACH) and only if there are no other more optimal lower risk clinical areas suitable for the respiratory pathway, then the NHS Boards should consider utilising the area for this purpose with provision of respiratory protective equipment (RPE) (FFP3 respirators) for the staff working in this area.
The evidence continues to support the most likely route of COVID-19 transmission being via the droplet and contact route. However, it is accepted that in some high risk environments housing COVID-19 cases where mitigations in line with the hierarchy of controls cannot be applied, the level of risk is unknown and as a precautionary approach, the use of RPE by staff in the designated area may be considered by the organisation. This takes account of guidance issued by the World Health Organization (WHO) occupational health and safety for healthcare workers
5.3.1 Ventilation in health and care settings
Adequate ventilation reduces how much infectious particles are in the air by dilution. It helps reduce the risk of transmission of respiratory pathogens - the risk is greater in areas that are poorly ventilated. This guidance document is not intended to contain technical detail on ventilation but rather provide over-arching advice on the considerations for health and care settings in the context of respiratory pathogens and risk reduction. The content below should be read in conjunction with the relevant national guidance relating to ventilation in the built environment.
A number of studies have linked COVID-19 transmission to recirculating air conditioners, with the high velocities created by these units potentially allowing larger viral aerosols to remain airborne over longer distances. It is also possible that directional flow from desk fans could have a similar effect however the evidence of this is weak. Fans should be avoided as much as possible and should not be used without prior risk assessment. An SBAR details the considerations for risk assessing fan use.
(SHTM 03-01 Part A) Ventilation for Healthcare - Design and validation details the ventilation requirements for healthcare settings and notes that 6 ACH is considered adequate for general areas within health and care settings across both the respiratory and non-respiratory pathways. Some areas of healthcare e.g. theatres, treatment rooms, dental surgeries require higher specification of mechanical ventilation and further details can be found in guidance laid out in section 5.3.2. Dental settings may also refer to SDCEP Ventilation Information for Dentistry. It is recognised that many health and care areas are not installed with mechanical ventilation systems to achieve a minimum of 6 ACH and NHS Boards/care providers are not required to upgrade ventilation throughout all of their estate (unless this is part of the existing strategic plans) however it should be noted that where mechanical ventilation provides 6ACH or more, that respiratory pathogen transmission risk is reduced. Other mitigations must be in place to reduce transmission risk such as those described in the hierarchy of controls in particular where there is no mechanical ventilation.
Service users with known or suspected respiratory viruses must not be placed in a positive pressure room.
5.3.2 Mechanically ventilated areas
NHS Scotland Boards/Health and Social care providers should seek assurance that their ventilation systems comply with guidance to which they were designed, including:
- Best practice guidance for healthcare engineering policies and principles (SHTM 00)
- Ventilation for Healthcare - Design and validation (SHTM 03-01 Part A)
- SHPN 36 Part 2 NHS Dental Practices in Scotland
Ensure ventilation systems are well maintained ensuring functionality of air handling units and correct delivery of assigned air change rates. Controls should be set to maximise the amount of fresh air coming into the space and avoid recirculation of air as much as possible. Dampers should also be opened as far as possible.
5.3.3 Naturally ventilated areas (No mechanical ventilation)
Ensure areas are ventilated as much as and as frequently as possible by opening windows if temperature/weather conditions allow. Where weather conditions do not allow for windows being opened, consider if other mitigations can be applied within the area to reduce risk. Organisations should consider any other safety risks with opening the windows where adjacent building works are in progress. If possible, open windows at different sides to get a cross flow of ventilation. Where it is safe to do so, doors may be opened. NB fire doors must NEVER be propped open. Airing rooms as frequently as permitted will help improve ventilation. Where only natural ventilation exists, ensure maximum application of other mitigations measures as far as possible aligned to the Hierarchy of Controls.
Aerosol Generating Procedures (AGPs) undertaken on service users with suspected/known respiratory viruses/infection should be avoided in rooms with less than 6ACH and this includes rooms limited to natural ventilation. If this cannot be avoided then a single side room should be used with all staff wearing appropriate airborne PPE, AGP fallow times adhered to and ensuring the door remains closed during the AGP and resulting AGP fallow time.
5.3.4 Air scrubbers
Where air-supply systems to high-risk clinical settings (in the context of respiratory transmission) are suboptimal, following risk assessment including assurance of the efficacy and safety of the filtration unit, health and care settings may consider using portable industrial grade air filtration units containing HEPA filters. As yet, evidence on the use of air scrubbers is limited and as such these should be used with caution. The units should be capable of recirculating all of the room air, without interfering with the existing pressure differential of the room and should provide a minimum of 6 air changes per hour. The unit must be sized appropriately for the room in which it will be utilised and maintenance contracts should be procured to accompany the unit. It should be noted that these units do not provide additional fresh air into a space and there is no standard to measure the efficacy of these devices. NHS Boards should satisfy themselves that these devices are suitable and if required, seek advice from estates departments. Boards should also assess (not limited to) the noise levels, power requirements, heat gains and potential trip hazards as part of the risk assessment.
Currently, the CIBSE and SAGE resources below provide the best available independent views of air cleaning devices.
“Air purifiers” are typically used in domestic settings and should not be used in health and care settings.
More information on ventilation in the context of COVID-19 can be found at the following resources;
CIBSE: Covid-19 Guidance: Ventilation
SAGE: Role of ventilation in controlling SARS-CoV-2
SAGE: Potential applications of air cleaning devices
5.3.5 Bed and treatment chair spacing
As a minimum, spacing in an area must allow for adequate physical distancing between service users across all facilities (unless physical distancing is not required e.g. residential settings) to help minimise transmission risk associated with respiratory viruses. However, it should be noted that physical distancing has been implemented as a pandemic measure and is considered separate from bed spacing guidance. All NHS boards and care providers must still aim to meet the minimum bed spacing requirements laid out in the guidance below for secondary care settings. This takes account of ergonomics within the clinical environment and not just healthcare associated infection (HAI) risk. Some other health and care settings may choose to adopt this guidance e.g. hospice settings.
 Dental settings
Dental settings
Since 2014, HBN 00-03’s Figure 45 states a day treatment bay should achieve 2.45m width / centre-to-centre dimension. IM/2020/024 & its supplementary SIM2108 Fig 2B, assume a 0.5m diameter zone for the patient head and up to 3 trolley/ couch/ chair(s) in a row, will achieve a 2m physical distancing, i.e. a minimum 2.5m centre-to-centre.

-
Secondary care settings
- Guidance consistently recognises that bed spacing requirements contribute towards the control of HAIs. Adult in-patient facilities designed post 2010 should achieve 3.6m (width) x 3.7m (depth) dimensions of SHPN 04-01, HBN 00-03 and SHFN 30. Width of 3.6m is measured from bed centre to bed centre.Since 2014, HBN 00-03’s Figure 45 states a day treatment bay should achieve 2.45m width / centre-to-centre dimension. IM/2020/024 & its supplementary SIM2108 Fig 2B, assume a 0.5m diameter zone for the patient head and up to 3 trolley/ couch/ chair(s) in a row, will achieve a 2m physical distancing, i.e. a minimum 2.5m centre-to-centre.For older facilities, designed post 1995, HBN 40 bed bay minimum of 2.7 x 2.9m, the preferred minimum bed centre is 2.9m. Facilities designed pre 1995, or for clinical specialties e.g. Mental Health (SHPN 35 / HBN 03-01) or Care of Older People (HBN 37), had a bed bay minimum of 2.4 x 2.9m. For this specific group, the pragmatic minimum of 2.7m bed centres should be adhered to, and/or reduction to total patient numbers/ occupation per multi-bed room and ventilation enhancements should be considered where practicable.Current NHS Scotland Guidance on bed spacing include:
- Core guidance - General design for healthcare buildings (HBN 00-01)
- Core guidance - Clinical and clinical support spaces (HBN 00-03)
- Critical care units (HBN 04-02)
- HAI-SCRIBE Manual information for project teams (SHFN 30 Part A)
- HAI-SCRIBE Implementation strategy and assessment process (SHFN 30 Part B)
- HAI-SCRIBE question sets and checklists (SHFN 30 Part C)
- Adult in-patient facilities (SHPN 04-01)
- In-patient accommodation - supp 1 - Isolation facilities in acute settings (SHPN 4 sup 1)
- Guidance consistently recognises that bed spacing requirements contribute towards the control of HAIs. Adult in-patient facilities designed post 2010 should achieve 3.6m (width) x 3.7m (depth) dimensions of SHPN 04-01, HBN 00-03 and SHFN 30. Width of 3.6m is measured from bed centre to bed centre.Since 2014, HBN 00-03’s Figure 45 states a day treatment bay should achieve 2.45m width / centre-to-centre dimension. IM/2020/024 & its supplementary SIM2108 Fig 2B, assume a 0.5m diameter zone for the patient head and up to 3 trolley/ couch/ chair(s) in a row, will achieve a 2m physical distancing, i.e. a minimum 2.5m centre-to-centre.For older facilities, designed post 1995, HBN 40 bed bay minimum of 2.7 x 2.9m, the preferred minimum bed centre is 2.9m. Facilities designed pre 1995, or for clinical specialties e.g. Mental Health (SHPN 35 / HBN 03-01) or Care of Older People (HBN 37), had a bed bay minimum of 2.4 x 2.9m. For this specific group, the pragmatic minimum of 2.7m bed centres should be adhered to, and/or reduction to total patient numbers/ occupation per multi-bed room and ventilation enhancements should be considered where practicable.Current NHS Scotland Guidance on bed spacing include:
Health Facilities Scotland have undertaken an assessment of bed and chair spacing within NHS Scotland facilities taking account of compounding factors applied in conjunction with physical distancing. The purpose of this document aims to help support boards in reviewing bed spacing to ensure 2 metre (m) physical distancing can be maintained for inpatient beds and treatment chairs. The summary document and the detailed technical diagrams can be accessed here including;
SIM2108 - COVID-19 Social Distancing Diagrams & Information , 12 July 2021NHSS Social Distancing Guidance & Signage (nhsnss.org) DL(2021)09 & NSS, 29 Jan 21NHS Scotland COVID-19 remobilisation –Built Environment incl. physical distancing support diagrams (IM/2020/024), 18 Sep 20
Draft 5.4 Physical distancing
The full guidance requirements for physical distancing are laid out in Appendix 18 of the NIPCM.
A summary of the key points is below;
- Physical distancing of 2m must remain for
- all inpatient areas (respiratory AND non-respiratory pathway),
- the respiratory pathway across all health and care settings
- outpatient departments (OPDs) which deliver treatments for extended periods of time throughout the day e.g. oncology units, renal dialysis units, recovery areas, day surgery
- for staff across all health and care settings when Type IIR Fluid Resistant Surgical Masks (FRSMs) are removed
- Physical distancing may be reduced across all other health and care settings not described above to 1 metre or more
- Service users who share living accommodation (care homes) do not need to physically distance from each other
- Any service user answering yes to any of the respiratory screening questions should be placed in the respiratory pathway which will remain at 2 metres physical distancing
- Physical distancing may be reduced amongst staff to 1 metre or more when Type IIR FRSMs are in use. If Type IIR FRSMs are removed for any reason e.g eating, drinking, it is advised that 2 metres or more be maintained to avoid high numbers of staff being identified as contacts should a positive case arise
- Physical distancing may be reduced amongst visitors to 1 metre or more. (see exceptions within Appendix 18 allowing visitors to hug/kiss loved ones)
- These changes to physical distancing do NOT mean a return to pre pandemic practices. Health and care settings must continue to adapt processes to ensure risk of transmission is minimised
- This is the minimum guidance – where clinical teams or care teams decide that maintaining 2 metres physical distancing throughout the department is necessary then they may do so.
Draft 5.5 General Infection Prevention and Control Information
SICPs covered in this chapter are to be used by all staff, in all health and care settings, at all times, for all service users whether infection is known to be present or not to ensure the safety of those being cared for, staff and visitors in the care environment.
SICPs are the basic infection prevention and control measures necessary to reduce the risk of transmission of infectious agent from both recognised and unrecognised sources of infection. More information can be found in chapter 1 of the NIPCM.
SICPs may be insufficient to prevent cross transmission of specific infectious agents. Therefore, additional TBPs are required to be used by staff when caring for service users with a known or suspected infection or colonisation. More information can be found in chapter 2 of the NIPCM.

Care Home Settings
Care homes can find more information on SICPs and TBPs specific to the care home setting within the Care home IPCM.
The additional TBPs required for different infectious pathogens vary depending on the route by which they are transmitted. Respiratory pathogens can be transmitted by the following;
- Contact transmission
- Droplet transmission
- Airborne transmission
The NIPCM also contains an A-Z list of pathogens and stipulates the mode of transmission for each.
Draft 5.6 Case definitions and symptomology
5.6.1 Definition of a confirmed COVID-19 case
5.6.2 Definition of a probable COVID-19 case
5.6.3 Definition of a possible COVID-19 case
Case definitions for COVID-19 have been widely used throughout the course of the pandemic and these will continue to be used going forward.
Establishing which symptoms are a result of COVID-19 and which symptoms are a result of another respiratory virus is often not possible. Respiratory testing is the only way to identify the causative pathogen.
The case definitions being used across the UK reflects current understanding from the epidemiology available and may be subject to change. Case definitions can be found below.
Please note: Beyond recommending a confirmatory PCR for probable and possible cases, from an IPC management perspective, there is no difference between how a possible, probable or a confirmed case of COVID-19 is to be managed. Contact tracing should take place after a positive Lateral Flow Device (LFD) test, i.e. a probable COVID-19 case.
5.6.1 Definition of a confirmed COVID-19 case
A person with laboratory confirmed detection of SARS-CoV-2 by PCR in a clinical specimen
Things to note:
- It is important to know where a PCR test is processed (e.g. tests may have been carried out in non-NHS laboratories. A list of non-NHS laboratories which have agreements in place with their local NHS laboratory can be accessed by emailing nlpq@nhs.scot). Results from non-NHS laboratories that are not aligned with their local NHS laboratories or UK-accredited need to be risk assessed or the test repeated.
- A positive PCR test may be due to fragments of the virus being present following infection in the previous 90 days
5.6.2 Definition of a probable COVID-19 case
A person with a positive LFD test.
5.6.3 Definition of a possible COVID-19 case
A person presenting recent onset of one or more of the following cardinal COVID-19 symptoms:
- new continuous cough
- fever/temperature ≥37.8°C
- loss of, or change in, sense of smell (anosmia) or taste (ageusia).
A wide variety of additional clinical signs and symptoms have also been associated with COVID-19. Fever may not be reported in all symptomatic people and cases may also be asymptomatic. It is important to take into account atypical and non-specific presentations in older people with frailty, those with pre-existing conditions and those who are immunocompromised. (further information on presentations and management of COVID-19 in older people and Scottish Government and Appendix 1 :Think COVID:Covid-19 Assessment in the Older Adult - Checklist).
Individuals must be assessed for bacterial sepsis or other causes of symptoms as appropriate.
5.6.4 Symptoms associated with other respiratory pathogens (Some of these symptoms will occur in individuals with COVID-19)
There are a number of symptoms associated with respiratory infection and the most common symptoms are listed below;
- Pyrexia (fever)
- Rhinorrhea (Runny nose)
- Congestion in the nasal sinuses or lungs
- Sore throat
- Cephalgia (headache)
- Coughing
- Sneezing
- Breathlessness
- Anosmia (Loss of sense of smell)
- Ageusia (Loss of sense of taste)
- Wheezing or chest tightness
- Myalgia (Muscle aches)
- Fatigue (Tiredness)
- Dyspnea (Shortness of breath)
These should be considered by clinicians’/care givers in conjunction with other underlying health conditions and any atypical symptoms associated with a possible respiratory virus/infection to determine whether the service user may have a respiratory pathogen requiring application of TBPs.
Draft 5.7 Respiratory screening assessment to determine transmission risk
The process of respiratory screening assessment will vary dependant on both the health and care facility and the type of service provision but wherever possible, respiratory screening questions should be undertaken by telephone prior to an arranged arrival at the facility for all service users and any accompanying carers . If this is not possible, then these questions should be asked on arrival at reception. This will help inform the clinical/care team of service user respiratory status and potential associated risk before face to face consultation should this be deemed appropriate. If respiratory screening is undertaken prior to arrival at a health and care facility, and if the service user answers ‘no’ to all of the respiratory screening questions, the service user should be reminded to inform a staff member should any symptoms develop prior to attendance at the facility. If the service user answers ‘Yes’ to any of the COVID-19 or the respiratory symptoms questions, place on the respiratory pathway. If the service user advises of having had a test positive pathogen in the last 14 days, they should be placed according to the infective period for that specific pathogen and an assessment of any ongoing infectivity. Refer to A-Z of pathogens for details of individual pathogens.
A word version of the respiratory screening questions is available.
Table 2: Respiratory Screening Questions for use across all health and care settings*
The screening questions below apply to all service users and anyone accompanying the service user to a healthcare facility e.g. parent, carer.
COVID-19 Screening questions |
Yes |
No |
|---|---|---|
| Do you or any member of your household/family have a confirmed diagnosis of COVID-19 diagnosed in the last 14 days? NB: Any person who has previously tested positive for SARS-CoV-2 by PCR should be exempt from being re-tested within a period of 90 days from their initial symptom onset, or the first positive test, if asymptomatic, unless they develop new possible COVID-19 symptoms. This is because fragments of inactive virus can be persistently detected by PCR in respiratory tract samples for some time following infection. |
||
| Do you or any member of your household/family have suspected COVID-19 and are waiting for a COVID-19 test result? | ||
| Have you travelled internationally in the last 10 days to a country that is on the Government red list? | ||
| Have you had contact with someone with a confirmed diagnosis of COVID-19, or been in isolation with a suspected case in the last 10 days? | ||
Do you have any of the following symptoms;
|
If the service user answers ‘Yes’ to any of the COVID-19 screening questions above, place on the respiratory pathway.
If service user answers ‘No’ to all of the COVID-19 screening questions above, proceed to general respiratory screening questions below.
General respiratory screening questions |
Yes |
No |
|---|---|---|
|
Do you have any new or worsening respiratory symptoms not already mentioned which suggest you may have a respiratory virus? (1 See note below) |
||
| Have you been had a laboratory test with a confirmed respiratory virus/infection such as Influenza in the last 14 days?2 |
If the service user answers ‘Yes’ to any of the COVID-19 or the respiratory symptoms questions, place on the respiratory pathway.
Notes
* COVID-19 screening questions are separated to recognise potential asymptomatic carriage of this pathogen. The screening questions above also apply to anyone accompanying the service user to a healthcare facility e.g. parent, carer.
1Note for healthcare workers (HCWs) in relation to respiratory symptoms;
List of respiratory symptoms below may indicate a respiratory virus;
-
-
- Rhinorrhea (Runny nose)
- Congestion in the nasal sinuses or lungs
- Sore throat
- Sneezing
- Coughing
-
The following can also be symptoms of a respiratory virus/infection but may also be related to a non-respiratory cause therefore caution should be applied in allocation of these patients to the respiratory pathway in the absence of any symptoms noted above.
-
-
- Breathlessness
- Wheezing or chest tightness
- Myalgia (Muscle aches)
- Fatigue (Tiredness)
- Dyspnea (Shortness of breath)
-
2 If the service user advises of having had a test positive pathogen in the last 14 days, they should be placed according to the infective period for that specific pathogen and an assessment of any ongoing infectivity. Refer to A-Z of pathogens for details of individual pathogens.
* COVID-19 screening questions are separated to recognise potential asymptomatic carriage of this pathogen. The screening questions above also apply to anyone accompanying the service user to a healthcare facility e.g. parent, carer.
It may also be useful to collect information on the service user’s vaccination status including the date vaccination was received if available.
 Primary Care and Community Health and Social Care settings
Primary Care and Community Health and Social Care settings
Respiratory screening questions & triage
If following telephone consultation, the individual is suspected or confirmed as having COVID-19 or another respiratory virus, and if the matter is non urgent, face to face consultation should be deferred until the COVID-19 self-isolation period has elapsed.
For other non COVID-19 respiratory viruses, defer until resolution of symptoms.Health and care professionals should see individuals face to face or via remote consultation, whichever is felt most appropriate where they have deemed further clinical assessment is required. If it is necessary to review the individual by means of a face to face consultation (regardless of the presenting problem) then they should be advised of the most suitable way to transfer to the facility, enter the health and care facility, and on arrival, should be directed to a suitable waiting area identified for symptomatic individuals.
NB: children with mild bronchiolitis and lower respiratory tract infections should be managed in primary care settings where possible to ensure a holistic primary care assessment. Planning should include the implementation of locally appropriate models of care enabling secondary care clinicians to support primary care colleagues. The expectation should be that children with mild and moderate bronchiolitis or lower respiratory tract infection are initially reviewed in primary care settings.
Entrances to facilities must clearly display the requirement for individuals entering the facility to don a face covering, maintain physical distancing and alcohol based hand rub (ABHR) should be provided for use prior to entry for those who are able to do so.
Respiratory screening questions should be undertaken on arrival at the facility if not carried out prior. For unplanned arrivals, respiratory screening questions should be completed immediately on arrival to the facility, where it is safe to do so without delaying any necessary immediate lifesaving interventions.
If providing a home visit, staff should contact the individual by telephone at home prior to the visit to undertake the respiratory screening if time allows. These should be repeated on arrival at the individual’s home. If an individual lacks ability to answer questions by telephone, an assessment should be made on arrival keeping 1 metre from the individual where possible ensuring that a Type IIR FRSM is worn. If this is not possible, treat as having respiratory symptoms until a direct assessment can be made by the care provider.
Only the individual requiring a consultation should attend health and care facilities unless a carer or escort is required.
Individuals living in residential facilities should be closely monitored for onset of respiratory symptoms by local care staff.
 Dental settings – Respiratory screening questions & triage
Dental settings – Respiratory screening questions & triage
If following telephone consultation, the patient is suspected or confirmed as having COVID-19 or another respiratory infection, and if the matter is non urgent, face to face consultation should be deferred until the COVID-19 self isolation period has elapsed. For other non COVID-19 respiratory viruses, defer until resolution of symptoms. If the matter is urgent, the patient may be seen within the dental setting but ideally should be provided with an appointment at the end of the day/session to reduce any post Aerosol Generating Procedure (AGP) fallow time (if an AGP is performed) impacting on the remaining patient consultation list.See section 5.15.6 Determining the IPC precautions required for AGPs.
 Secondary Care settings
Secondary Care settings
Respiratory screening and triage questions
Patients should be assessed for respiratory symptoms at the earliest opportunity to direct them to the safest route within the facility.SAS staff should undertake the respiratory screening questions prior to arrival at the receiving Emergency Department and accompany the patient to the appropriate waiting area dependant on outcome.It is recognised that patient placement will be dependent on clinical need in addition to respiratory status. Where a patient with respiratory symptoms cannot be placed in the respiratory cohort for clinical reasons, avoid placing the patient next to anyone high risk and previously considered to be on the shielding list, keep curtains pulled as a physical barrier if safe to do so and ensure thorough cleaning as per respiratory care pathway described in the environmental cleaning section.
Reception areas must display signage encouraging service users to report respiratory symptoms immediately on arrival and reception staff should ask all service users on arrival using the respiratory screening questions regardless of the reason for presentation at the facility and where it is safe to do so without delaying any lifesaving interventions. Service users who answer YES to any of the questions should be directed to the appropriate waiting area and the receiving clinical staff alerted to their presenting respiratory symptoms.
Only the service user requiring a consultation should attend health and care facilities unless a carer or escort is required.
Draft 5.8 Placement and management of a service user with respiratory symptoms
5.8.2 Transfer of service users with respiratory symptoms/confirmed respiratory pathogen
The COVID-19 patient pathways/categories will now be replaced with a respiratory pathway. This is determined as a route to which patients symptomatic of respiratory infection should be directed.
A respiratory assessment algorithm is available to help determine which pathway the service user should be placed on and whether or not TBPs should be applied.
The pathway should be further split into appropriate cohorts determined by presenting symptoms and when available, test results to determine the causative pathogen.
Entrances to facilities must clearly display the requirement for individuals entering the facility to don a face covering, maintain physical distancing and alcohol based hand rub (ABHR) should be provided for use prior to entry for those who are able to do so.
Waiting areas should be segregated with an area set aside for use by service users who present with respiratory symptoms. Markers to identify segregation should be clear and service users must be advised not to circulate around waiting areas and remain seated until called .
Cleaning within waiting areas segregated for respiratory patients should be undertaken as laid out in environmental cleaning section.
Removing toys and books may help prevent children circulating in these areas and instead parents may be advised to bring a toy or book belonging to the child to help keep them occupied during the wait time. Children should be supported by parents/carers with hand and respiratory hygiene.
Members of the same family/household do not need to physically distance in waiting areas.
Please note that prior to undertaking aerosol generating procedures (AGPs) on the non-respiratory pathway, airborne precautions are still required for service users unless there is evidence of a negative COVID-19 test within the preceding 48 hours. See section 5.15.6 Determining the IPC precautions required for AGPs.
 Primary Care and Community Health and Social Care settings
Primary Care and Community Health and Social Care settings
Patient/Individual Service user placement
Health and care facilities should identify in advance areas/routes/consultation rooms for individuals who are displaying respiratory symptoms and who have been assessed as requiring a face to face consultation. It is recognised that some small practices will not have space to facilitate separate waiting areas for individuals on the respiratory pathway. In this case, a local risk assessment should be undertaken to determine how best to manage these individuals and whether it is suitable for them to attend for face to face consultations.
Where possible, consultation/treatment rooms should be identified for placement of individuals with respiratory symptoms. Some health and care facilities may be very small with limited consultation rooms and the ability to dedicate a room to respiratory individuals may not be possible. If this is the case, consider allocating respiratory cases to the end of a session. Ensure cleaning of touch surfaces within the consultation room is undertaken thoroughly immediately after the patient/individual leaves the room. Particular attention should be paid to anything touched by the individual and anything within short range of individuals who are coughing/sneezing.
Individual Service user placement in residential facilities
All admissions from the community to a residential health and care setting should be assessed first by the health and care setting using the respiratory screening questions. This applies to all types of residential heath and care setting admissions (including for respite).
For those residents who are displaying respiratory symptoms, the admission should be delayed if possible until they have completed their COVID-19 self-isolation period, OR if COVID-19 negative, until symptoms are resolving.
Conduct a local risk assessment if the admission cannot be delayed to ensure it is done safely. See PHS Social Care and Residential Care COVID-19 guidance for further information on admissions to these settings including for respite.
If the admission must go ahead, the resident should be allocated their own room preferably with en suite facilities.
Meals should be provided for the resident to eat within their room to avoid them entering any communal spaces.
Ensure that personal toiletries such as towels (unless laundered to a satisfactory standard between individuals) toothbrushes and razors are not shared. Consider a rota for showering and bathing placing the resident with respiratory symptoms last.
Only essential staff wearing appropriate PPE should enter the rooms of residents with respiratory symptoms. All necessary care should be carried out within the resident’s room.

Dental settings - Patient/Service user placement
Where possible, waiting areas should be segregated with an area set aside for use by patients who present with respiratory symptoms. Markers to identify segregation should be clear and patients must be advised not to circulate around waiting areas and remain seated until called. Members of the same family/household do not need to physically distance in waiting areas. Cleaning within areas segregated for respiratory patients should be undertaken as per guidance laid out in environmental cleaning section.
It is recognised that some small practices will not have space to facilitate separate waiting areas for patients on the respiratory pathway. In this case, a local risk assessment should be undertaken to determine how best to manage these patients e.g. wait in car until called or schedule for end of a session, or whether it is suitable for them to attend for face to face consultations.
Dental services should identify in advance areas/routes/consultation rooms for patients who are displaying respiratory symptoms and who have been assessed as requiring treatment. Ideally, these patients should be seen at the end of the day/session to reduce any post Aerosol Generating Procedure (AGP) fallow time (if an AGP is performed) impacting on the remaining patient consultation list.Where space allows, a dedicated consultation/treatment rooms should be identified for placement of patients with respiratory symptoms. Some dental practices may be very small with limited consultation rooms and the ability to dedicate a room to respiratory patients may not be possible.
 Secondary care settings
Secondary care settings
Inpatient placement
At the point of admission to the facility it is unlikely to be known what pathogen is the cause of respiratory symptoms. Respiratory pathways should be developed in hospitals in a bid to separate patients with suspected/confirmed respiratory viruses from all other patients as far as possible. Respiratory pathways may be dedicated wards or dedicated bed bays within wards. Patients with suspected or known respiratory viruses should be placed in a single side room. Where single side rooms facilities are lacking, patients with the same confirmed pathogen should be cohorted together.Where test results are not yet available to determine the viral pathogen causing the respiratory symptoms it may be necessary to cohort suspected respiratory infections together in the same multi bed bay. NB: This carries the risk of transmitting multiple respiratory viruses to multiple patients and should be avoided wherever possible and only used as a last resort during times of extreme bed pressures.The following principles should be followed when considering cohorting of respiratory cases still awaiting test results;
-
-
- Ensure a respiratory screen including COVID-19 has been undertaken ideally prior to entry into the cohort or at the earliest opportunity.
- Ensure the beds within the multi bedded area are adequately spaced
- Ensure patients are provided with a Type IIR FRSM to wear where tolerated
- Ensure there are adequate hand hygiene facilities for staff and patients
- Advise all patients to remain within their bed space at all times
- Ensure patients are advised of good respiratory etiquette and are provided with tissues and waste disposal bags.
- Where safe to do so, curtains could be drawn between patients to create a barrier
-
Patients who should not be placed in multi bed bay cohorts;
-
-
- Patients considered high risk and previously on shielding list
- Patients undergoing an AGP
- Patients known to have another known infectious pathogen or symptoms of a suspected infectious pathogen e.g. C.difficile, Norovirus, loose stools, MRSA
- Patients who are unlikely to comply with the requirements of the cohort described above
-
Patients with respiratory symptoms who require AGPs should be prioritised for a single side room. Critical care areas and wards where AGPs are undertaken more routinely should also prioritise single side rooms for those with respiratory symptoms undergoing AGPs. However, where single side room capacity is lacking and patients with respiratory symptoms on the unit increases, unit-wide application of airborne precautions should be considered where all the patients in the same bed bay are test positive for the same respiratory pathogen. Where patients are positive for different respiratory pathogens there is a risk of transmission of multiple pathogens to multiple patients.
Paediatric inpatient placement
The principles applied within this guidance aim to mitigate the risk of transmission of all respiratory viruses including RSV. The UK is experiencing a surge in RSV cases amongst the paediatric population and winter season and has commenced earlier than previous years. Many paediatric settings will have well established RSV pathways. Wherever possible, both COVID-19 and RSV point of care testing should be undertaken as a minimum on admission to help allocate patient placement and ensure that cohorts of RSV are segregated from cohorts of COVID-19. See also cohorting principles for secondary care inpatients above. Regardless of the infectious pathogen detected, whilst the patient is symptomatic, they should be managed in line with the TBPs within this guidance. If single room capacity is limited/ being exceeded, prioritise clinically vulnerable children to a single room (See RCPCH guidance on clinically extremely vulnerable children). Children with bronchiolitis requiring a continuous AGP should be prioritised to a single room over those not requiring a continuous AGP if possible.When children require an inpatient stay, local policy should be followed regarding resident carers. Education and written information for resident carers should be made available regarding respiratory virus, local policies, and include use of communal facilities, face coverings (unless exempt), hand hygiene, PPE and physical distancing.
Elective care pre-admission planning
Whilst the COVID-19 pandemic continues, it is important that any risk associated with acquiring COVID-19 pre/intra/post operatively for patients being admitted for elective surgical procedures be reduced as far as possible. Some studies have shown that patients diagnosed with COVID-19 around the time of a surgical procedure have a higher than predicted mortality however, it is not possible to determine precise risk for each individual patient. In advance of patients attending for elective surgery they should be advised of ways in which they may be able to reduce their post-operative risk. The following patient information leaflet explains some of the risk reduction measures and can be provided to patients in advance of their planned admission alongside testing advice. Appendix 19 of the NIPCM provides details of Elective Surgery IPC principles which have been developed in conjunction with the Scottish COVID-19 Clinical cell and aim to reduce COVID-19 transmission risk during the ongoing COVID-19 pandemic. These should be read alongside the patient information leaflet accessed here.
 Care Home Settings
Care Home Settings
Admissions and resident placement
Full guidance for admission to a care home during the COVID-19 pandemic can be found in PHS COVID-19: Information and Guidance for Care Home Settings (Adults and Older People).
Any resident who answers yes to any of the respiratory screening questions should be placed in their own individual room until a full assessment can take place to determine the cause.
Where single rooms are limited cohorting may be considered. Cohorting in care homes should be undertaken with care. Residents who are high risk and previously considered to be on the shielding list must not be placed in cohorts and should be prioritised for single occupancy rooms.
Where all single room facilities are occupied and cohorting is unavoidable, then cohorting could be considered in conjunction with the local Health Protection Team (HPT).
-
-
- Residents who are awaiting test results to confirm which pathogen is causing respiratory symptoms, should not be placed together in cohorts if at all possible
- Ensure a respiratory screen including COVID-19 has been undertaken ideally prior to entry into the cohort or at the earliest opportunity.
- Ensure residents are provided with a Type IIR FRSM to wear where tolerated
-
5.8.1 Staff cohorting
Efforts should be made as far as reasonably practicable to dedicate assigned teams of staff to care for service users on the respiratory pathways where TBPs are applied.
There should be as much consistency in staff allocation as possible, reducing movement of staff and the crossover between the respiratory pathway and all other service users.
Rotas should be planned in advance wherever possible, to take account of the respiratory pathway and staff allocation.
For staff groups who need to go between pathways, efforts should be made to see service users on the non-respiratory pathway first.
Type IIR FRSMs should be changed if wet, damaged, soiled or uncomfortable and must be changed after having provided care for a service user with any other suspected or known infectious pathogens and when leaving respiratory pathway areas.
5.8.2 Transfer of service users with respiratory symptoms/confirmed respiratory pathogen
Wherever possible, service users with respiratory symptoms or a confirmed respiratory pathogen should remain on the respiratory pathway until they meet criteria for discontinuation of precautions. There may however be instances where it is necessary to transfer a service user whilst TBPs are ongoing including;
- The service user no longer requires critical care and the critical care bed is required for another patient
- The service user requires escalation of care to a secondary care facility or a critical care unit
- The service user requires urgent treatment in a regional specialist unit and postponement would have a detrimental effect on the patient and the care cannot be provided on the ward they currently reside in
- The service user requires an urgent procedure or investigation to be undertaken and postponement would have a detrimental effect on the individual
Communication with the receiving department/NHS Board/Care provider is vital to ensure appropriate IPC measures are continued during and after transfer. The service user must continue to be managed on the respiratory pathway. Communications must include;
- Service user symptom onset date
- Service user positive test date (if confirmed)
- Causative pathogen if known
- Date when service user may discontinue TBPs
- Current symptom status and any test results still awaited
- Any service user details which prevent or impact on the TBPs required i.e. falls risk requiring door to remain open, service user does not adhere to isolation
- Confirm if local IPCT (or HPT where appropriate) has been informed of transfer
Ensure transferring ambulance or portering staff are advised of the necessary precautions required for PPE and decontamination of transfer equipment.
There is no need to test the service user again on transfer provided symptomatic cases have already had a test taken where the health and care setting has the ability to do so.
5.8.3 Day/Overnight Pass
Service users who have been allowed to leave the healthcare facility for the day or for an overnight stay should be assessed using the respiratory screening questions in advance of their immediate return to the facility and again on arrival at the facility to determine any known or potential exposure whilst out of the healthcare facility on pass and subsequently which pathway they should be placed on.
Draft 5.9 Respiratory testing for service users
5.9.2 Testing for other respiratory pathogens
In order to ensure prompt safe placement and treatment of service users with respiratory symptoms, testing will help to inform the clinical/care team of the causative pathogen. This will help to avoid placing multiple service users with different respiratory pathogens in the same room for extended periods of time risking transmission of multiple pathogens between service users. Testing for other respiratory pathogens beyond SARS-CoV-2 may not be routinely necessary in all settings such as residential care areas and care homes.
5.9.1 COVID-19 testing
COVID-19 testing must continue as part of the ongoing COVID-19 pandemic efforts.
Anyone who has previously tested positive for SARS-CoV-2 by PCR should be exempt from being re-tested within a period of 90 days from their initial symptom onset, or the first positive test, if asymptomatic, unless they develop new possible COVID-19 symptoms. This is because fragments of inactive virus can be persistently detected by PCR in respiratory tract samples for up to 90 days following infection.
If an asymptomatic person is inadvertently re-tested and tests positive by LFD or PCR within 90 days of a previous positive PCR result, a risk assessment will likely conclude there is no need to do a confirmatory PCR, isolate or contact trace again, as long as the person with the repeat positive test:
- remains asymptomatic;
- is not a contact of a confirmed case;
- is not required to isolate having returned from travel to a non-exempt country;
See section ** for determining the precautions required for AGPs and the associated testing.
 Primary Care and Community Health and Social Care settings
Primary Care and Community Health and Social Care settings
As part of the ‘Test and Protect’ approach, everyone with symptoms of COVID-19 is encouraged to get tested. Tests can be booked through NHS inform.
If an individual has COVID-19 symptoms they should visit the NHS inform website to arrange testing.
GPs who have arranged a face to face consultation with an individual who has symptoms of COVID-19 should advise that arrange to take a COVID-19 PCR test via NHS Inform if they have not already done so.

Dental settings – COVID-19 testing
As part of the ‘Test and Protect’ approach, everyone with symptoms of COVID-19 is encouraged to get tested. Tests can be booked through NHS inform. Dental teams who have arranged a face to face consultation with a patient which cannot be postponed and who has symptoms of COVID-19 should advise that they should arrange to undertake a COVID-19 PCR test via NHS Inform if they have not already done so. The patient must then follow the respiratory pathway.
 Secondary care Settings
Secondary care Settings
A letter was issued to NHS Scotland Chief Executives on 27th November 2020 detailing the staged roll out of admission testing expansion plan to include;
-
-
- All emergency admissions to hospitals
- All planned admissions to hospitals
- Routine testing of asymptomatic, patient facing healthcare workers (HCWs)
-
A table containing a summary of testing requirements in NHS Scotland is available. When using this table the following applies;
-
-
- Screening undertaken out with national programmes which are detailed at the links above should be based on decision of clinical services e.g. screening in critical care settings.
- Screening undertaken out with national programmes which are detailed at the links above should be based on decision of clinical services e.g. screening in critical care settings.
- It is recognised that a patient may meet different criteria for testing multiple times in a short period of time (admission screening, transfers to another ward, contact of a case, outbreak management). If an inpatient has undergone a COVID-19 test in the previous 24 hours, there is no need to repeat it and the result can be accepted for any of the testing requirements with the exception of
- New symptoms onset – a new test should be performed as soon as symptoms are recognised
- Pre elective screening – where the requirement for a negative test must be within a set time period.
-
Care home settings
Guidance on COVID-19 testing in care home settings can be found in the PHS COVID-19: Information and Guidance for Care Homes (Adults and Older People).
5.9.2 Testing for other respiratory pathogens
It may be necessary to test for other respiratory pathogens including COVID-19 to support service user placement but also ensure optimal treatment provision.
GPs may choose to perform a respiratory screen on an individual if clinical assessment indicates this is necessary. If so, they should continue to do so via routine processes. There is no expectation to perform respiratory testing in primary care, or dentistry beyond routine processes indicated by clinical assessment.
 Secondary Care settings
Secondary Care settings
On arrival at a secondary care facility, all patients should have a COVID-19 test undertaken even if asymptomatic. Where available, multiplex rapid testing should be undertaken (symptomatic patients only) to help determine patient placement within the respiratory pathway and establish patient cohorts where required. Clinical teams may choose to perform a full respiratory screen if clinical assessment indicates this is necessary to support diagnosis.
 Care Home Settings
Care Home Settings
Residents who test negative for COVID-19 but who have ongoing respiratory symptoms do not routinely require any additional testing. However, should a resident require a consultation with a GP, the GP may choose to perform a full respiratory screen if a clinical assessment indicates this is necessary. Or if there is considered to be a cluster of cases and these are COVID-19 negative then additional testing by multiplex PCR can be performed to identify the pathogen.
Where respiratory screens are performed and the service user tests positive for COVID-19 within 90 days of previous positive test, this will require careful consideration and interpretation by clinicians with microbiology support where required.
Draft 5.10 Respiratory Screening for Healthcare Workers (HCW)
Twice weekly LFD COVID-19 screening has been rolled out to all HCWs employed directly by NHS Scotland and NHS24 and SAS call handlers. More information can be found on the Scottish Government website.
There is no requirement for any other respiratory pathogen beyond COVID-19 screening amongst HCWs unless recommended by an Incident Management Team, HPT, or occupational health.
 Care home settings
Care home settings
Weekly care home staff PCR screening for COVID-19 remains in place. Weekly PCR testing is now achieved through Regional Hubs. Care home staff should use the COVID testing portal - see http://www.covidtestingportal.scot to arrange this.
Further information on COVID-19 testing amongst care home workers can be found in the PHS Care home guidance.
Draft 5.11 Duration of Transmission Based Precautions for respiratory pathogens (excl COVID-19)
Before control measures are stepped down for respiratory pathogens, clinical teams and care teams must first consider any ongoing need for TBPs necessary for any other alert organisms, e.g. MRSA carriage or C. difficile infection, or other symptoms suggestive of possible infection such as diarrhoea.
Appendix 11 of the NIPCM details the duration of TBPs required for individual pathogens. Clinical teams and care teams should refer to this before any TBPs are discontinued. Duration of precautions for COVID-19 are given in more detail. A more cautious approach is taken when considering when to discontinue precautions for individuals with COVID-19 during the ongoing pandemic.
Draft 5.12 - Duration of transmission based precautions for COVID-19
5.12.1 Non COVID-19 discharges from hospital to care homes
5.12.2 Management of contacts of COVID-19
5.12.3 HCWs isolation and exemption requirements
It is important to note that service users with COVID-19 deemed clinically fit for discharge can and should be discharged before resolution of symptoms.
The tables below set out number of isolation days required, the clinical requirements for discontinuing TBPs and any testing required.
Table 3: Duration of precautions for hospital inpatients remaining in hospital and residents in residential care areas
Hospital Inpatients and residents in residential settings |
Number of isolation days required |
COVID-19 Clinical requirement for stepdown |
Testing required for stepdown |
|---|---|---|---|
General |
14 days from symptom onset (or first positive test if symptom onset undetermined) |
Clinical improvement with at least some respiratory recovery. Absence of fever (>37.8oC) for 48 hours without use of antipyretics. |
Not routinely required |
Individuals severely Immunocompromised as determined by Chapter 14a of the Green Book |
14 days from symptom onset (or first positive test if symptom onset undetermined) |
Clinical improvement with at least some respiratory recovery. Absence of fever (>37.8oC) for 48 hours without use of antipyretics. Individual risk assessment by clinical teams taking account of symptoms, clinical presentation, intended setting for stepdown. |
Local clinical teams may consider testing as part of the stepdown process and where undertaken, 1 negative test would be acceptable for stepdown. |
Individuals with severe COVID-19 (requiring ITU/HDU for COVID-19 treatment) |
14 days from symptom onset (or first positive test if symptom onset undetermined) |
Clinical improvement with at least some respiratory recovery. Absence of fever for 48 hours without use of antipyretics. Individual risk assessment by clinical teams taking account of symptoms, clinical presentation, intended setting for stepdown. |
Local clinical teams may consider testing as part of the stepdown process and where undertaken, 1 negative test would be acceptable for stepdown. |
Table 4: Stepdown requirements for inpatients being discharged from hospital
Discharging service users |
Number of isolation days required |
Does isolation need to be completed in hospital? |
COVID-19 Clinical requirement for stepdown |
Testing required for stepdown |
|---|---|---|---|---|
Patient discharging to a residential setting |
14 days from symptom onset (or first positive test if symptom onset undetermined). If they have completed the 14 day isolation in hospital, no further isolation should be required on return/admission to the care home. |
No. If a COVID-19 recovered patient is discharged to a care home before 14 day isolation has ended then 2 negative PCR tests are required before discharge at least 24 hr apart. If not completed 14 days isolation in hospital, they can do so in care home and do not require to start new isolation period on admission, nor require further testing. |
Clinical improvement with at least some respiratory recovery. Absence of fever for 48 hours without use of antipyretics |
If a COVID-19 recovered patient discharged to care home before 14 day isolation has ended then 2 negative PCR tests are required before discharge at least 24 hr apart. If not completed 14 days isolation in hospital, they can do so in care home and do not require to start new isolation period on admission, nor require further testing. See PHS COVID-19: information and guidance for care home settings for discharge testing details if the COVID-19 recovered patient has completed their 14 day isolation period in hospital |
|
Patients being discharged to their own home - General |
14 days from symptom onset (or first positive test if symptom onset undetermined) |
May complete at home and follow Stay at home guidance. Must be given clear advice for what to do if their symptoms worsen. |
Clinical improvement with at least some respiratory recovery. Absence of fever for 48 hours without use of antipyretics. |
Not routinely required |
|
Patients being discharged to their own home – someone in household is severely immunocompromised or at risk of severe illness |
14 days from symptom onset (or first positive test if symptom onset undetermined) |
Wherever possible, patient should be discharged to a different household from anyone immunocompromised or at severe risk of infection. If not possible – see ‘testing required for stepdown’ column. |
Clinical improvement with at least some respiratory recovery. Absence of fever for 48 hours without use of antipyretics. |
Testing for clearance is encouraged |
5.12.1 Non COVID-19 discharges from hospital to care homes
All non-COVID-19 residents being discharged from hospital should be isolated for 14 days from the date of discharge from hospital.
Risk assessment prior to hospital discharge for residents with a non-COVID-19 diagnosis should be undertaken in conjunction with the care home. A single negative result should be available preferably within 48 hours prior to discharge from hospital. The exception is where a resident is considered to suffer detrimental clinical consequence or distress if they were not able to be discharged to a care home. In these cases, the resident may be discharged to the care home prior to the test result being available, whether the result is positive or negative, but the 14 days of isolation must be completed regardless in the care home.
For further guidance on admission of COVID-19 recovered and non-COVID-19 residents from hospital or from community to a care home please refer to PHS COVID-19: Information and Guidance for Care Home Settings (Adults and Older People)
5.12.2 Management of contacts of COVID-19
Self isolation of contacts is no longer required in the general community if the individual is asymptomatic, doubly vaccinated with an MHRA approved vaccine and has a negative PCR test following the exposure to COVID-19. This does not apply to some health and care settings.
 Secondary care settings
Secondary care settings
Patients who have an overnight admission within a hospital setting who have been managed as a contact of a confirmed case of COVID-19 either
-
-
- during their hospital inpatient stay,
- in the community prior to admission to hospital
-
must isolate for 14 days whilst in hospital from the date of exposure to the COVID-19 case. If the patient is discharged to their own home within the 14 day self isolation period, individuals do not need to continue self-isolation provided they remain asymptomatic, have a negative PCR test after exposure to the case and are doubly vaccinated.
 Care home settings
Care home settings
Residential care settings and care homes will also still need to apply the 14 days’ self-isolation period for contacts of COVID-19 cases even if they meet the contact self-isolation exemption criteria. The 14 days period starts from the date of last exposure to the case and should be agreed between the hospital and care home manager, supported by HPTs and include an negative PCR test. This precautionary approach recognises the vulnerability of the other residents living in the care home.
5.12.3 HCWs isolation and exemption requirements
HCWs who test positive for COVID-19 on an LFD test must not report to work and must arrange to have a PCR test undertaken. If the positive LFD was undertaken whilst in the workplace, they must don a Type IIR FRSM (unless exempt), inform their line manager and go home immediately. If the PCR is COVID-19 positive, the HCW must self isolate at home for 10 days in line with advice on NHS inform.
Health and care staff who have been exposed to a case of COVID-19 should follow advice laid out in the Scottish Government DL (2021) 24 issued 27th August 2021.
If the PCR is COVID-19 negative, the HCW should consider the risk to service users if they are to return to work particularly if the service user they care for are immunosuppressed or otherwise medically vulnerable. If in doubt about any risk they may pose to patients or colleagues, this should be discussed with their line manager in the first instance.
Draft 5.13 - Hand Hygiene
Hand hygiene is considered one of the most important practices in preventing the onward transmission of any infectious agents including respiratory viruses. Hand hygiene should be performed in line with section 1.2 of SICPs. Within this section you will find videos demonstrating how to perform a hand wash and how to perform a hand rub.
 Care Homes
Care Homes
Staff in care homes settings can refer to the hand hygiene section of the Care Home IPCM (CHIPCM) for older people and adult care homes for more information and resources specific to this setting.
Draft 5.14 - Respiratory etiquette
Respiratory and cough hygiene is designed to minimise the risk of cross transmission of respiratory pathogens including COVID-19. The principles of respiratory and cough hygiene can be found in section 1.3 of SICPs.
The ‘Catch it, Bin it, Kill it’ poster can be downloaded.
 Care Homes
Care Homes
Staff in care homes settings can refer to the respiratory and cough hygiene section of the CH IPCM for older people and adult care homes for more information and resources specific to this setting.
Draft 5.15 - Personal Protective Equipment (PPE)
5.15.1 Extended use of face masks for staff, visitors and outpatients
5.15.2 Sessional use of FRSMs, FFP3 respirators and/or eye/face protection
5.15.3 Filter Face Piece 3 (FFP3) Respirators
5.15.4 PPE worn when caring for service users on the respiratory pathway
5.15.6 Aerosol Generating Procedures (AGPs)
PPE exists to provide the wearer with protection against any risks associated with the care task being undertaken. As part of SICPs, all staff undertaking in procedure, should assess any likely exposure and ensure PPE is worn that provides adequate protection against the risks associated with the procedure or task being undertaken. More information on PPE including donnng and doffing resources can be found in the NIPCM.
 Care home settings
Care home settings
Staff within Care Homes can find more general information on PPE in the CHIPCM for Older People and Adult Care Homes. Staff in care homes must follow the PPE guidance below.
When caring for a service user who has respiratory symptoms PPE should be selected to protect against droplet or in some circumstances, airborne spread.
PPE must not be used inappropriately. It is of paramount importance that PPE is worn at the appropriate times, selected appropriately and donned and doffed properly to prevent transmission of infection.
PPE is the least effective control measure within the hierarchy of controls and other mitigation measures must be implemented and adhered to wherever possible.
5.15.1 Extended use of face masks for staff, visitors and outpatients
The extended use of facemasks by health and care workers and the wearing of face coverings by visitors and outpatients (unless exempt) is designed to protect staff and service users as part of the COVID-19 pandemic. This is because COVID-19 may be transmitted by individuals who are not displaying any symptoms of the illness (asymptomatic or pre-symptomatic).
- View further Scottish Government guidance and associated FAQs.
- View a poster detailing the ‘Dos and donts’ of wearing a face mask.
- View a poster that supports the wearing of a non-medical face mask/face covering.
In Scotland, staff are provided with Type IIR FRSM for use as part of the extended wearing of facemasks.
 Primary Care and Community Health and Social Care settings
Primary Care and Community Health and Social Care settings
Face coverings for Individuals and service users
Any service users attending a health and care facility must wear a face covering in line with Scottish Government guidance unless exempt. Type II FRSM should be available should an individual or service user attend without a face covering.

Dental settings
Any patient attending a health care facility must wear a face covering in line with Scottish Government guidance unless exempt. Type II FRSM should be available should a patient attend without a face covering.

Secondary care settings
Face masks for Inpatients
A facemask should be worn by all inpatients across all inpatient areas regardless of respiratory symptoms unless exempt and where it can be tolerated and does not compromise their clinical care for example when receiving oxygen therapy. All patients should be encouraged to adhere to this which is part of COVID-19 pandemic control measures. The purpose of this is to minimise the dispersal of respiratory secretions and reduce environmental contamination. This should be actively promoted throughout the healthcare setting.It is recognised that it will be impractical for inpatients to wear facemasks at all times and these will have to be removed for reasons such as eating and drinking or showering. There is no need for inpatients to wear a facemask when sleeping provided the beds are at least 2 metres apart.A facemask should be worn by all inpatients across all pathways during transfer between departments within the hospital unless exempt. Where an inpatient is isolated in a single room, they do not need to wear a facemask. However, the inpatient must be asked to don their mask when any staff or visitors enter the room and before they are within a 2 metre distance of the patient.
Care home settings
Face masks for residents
Residents on the respiratory pathway should be encouraged to wear a facemask, if these can be tolerated and do not compromise care, when moving around the care home and when care staff, other residents or visitors enter their individual room.
5.15.2 Sessional use of FRSMs, FFP3 respirators and/or eye/face protection
FRSMs and eye/face protection (goggles/visors) may be used sessionally. This means that FRSMs and eye/face protection (where required) can be used moving between service users and for a period of time where a HCW is undertaking duties in an environment where there is exposure to respiratory pathogens. A session ends when the healthcare worker leaves the clinical setting or exposure environment.
Typically, sessional use of any PPE is not permitted within health and care settings at any time as it is associated with transmission of infection between service users within health and care settings.
Due to the much wider and frequent use of FRSMs eye/face protection (where required) by HCWs during the ongoing COVID-19 pandemic and during periods of increased respiratory activity in health and care settings both as part of service user direct care delivery and extended use of facemasks policy, sessional use of FRSMs and eye/face protection is permitted at this time.
However, in using FRSMs/eye and face protection/RPE sessionally, it is important to note the following;
- FRSMs/FFP3 must be replaced if visibly contaminated, wet, damaged, uncomfortable, when moving between the respiratory and non-respiratory pathway
- Eye/face protection must be replaced if damaged, visibly contaminated, when moving between the respiratory and non-respiratory pathway
- HCWs must not touch their FRSM, eye/face protection or FFP3 respirator whilst in situ. If they inadvertently do so, they must perform hand hygiene immediately afterwards
The above measures in conjunction with safe donning and doffing of PPE ensure the safety of the HCW and the service user.
No other PPE is permitted to be worn sessionally moving between service users or care tasks. This includes gloves, aprons and gowns.

Dental settings
Sessional use of FRSMs, FFP3 respirators and/or eye face protection
Within dental settings, HCWs may wear FRSMs sessionally to account for the extended use of facemask policy outside of direct patient care delivery and provided they are changed at the points listed above. It should be noted that due to the procedures being undertaken in dentistry and the splash/spray generated during those procedures, that FRSMs should be changed between patients in line with standard practices. FFP3 respirators should not be worn sessionally at any time.

Secondary care settings
Sessional use of FFP3 respirators
Sessional use of FFP3 respirators is also permitted only where unit wide airborne precautions are applied throughout a unit/care area however all other AGP PPE should be removed when no longer within 2 metres of a patient or, if still within 2 metres of the patient, then after the AGP is complete and fallow time has elapsed. It is not necessary to wear sessional gowns moving around a unit or department. Gowns protect against excessive splash and spray which is associated with AGPs and other direct patient care procedures.
5.15.3 Filter Face Piece 3 (FFP3) Respirators
FFP3 respirators must only be worn by staff who have undergone and passed a fit test. FFP3 respirators must be worn by HCWs in the following scenarios;
- When performing an Aerosol Generating Procedure (AGP) a service user with a known or suspected respiratory infection and those on the non respiratory pathway where there is no evidence of a negative COVID-19 test in the preceding 48 hours. See section 5.15.6 Determining the IPC precautions required for AGPs.
- When working within the respiratory pathway where AGPs are being performed unit wide (service users having AGPs undertaken who cannot be placed in single isolation rooms)
- Secondary care only - When working in the respiratory pathway in a clinical area deemed as having an unacceptable risk of transmission by the NHS Board (see hierarchy of controls section)
More information can be found on RPE within chapter 2 of the NIPCM.
5.15.4 PPE worn when caring for service users on the respiratory pathway
Table 5 details the PPE which should be worn when providing direct care for service users on the respiratory pathway.
Type IIR FRSM should be worn for all direct care delivery regardless of whether the service user is on the respiratory pathway or not. This measure has been implemented alongside physical distancing specifically for the COVID-19 pandemic.
Type IIR FRSMs can be worn sessionally when going between service users on the respiratory pathway. Type IIR FRSMs should be changed if wet, damaged, soiled or uncomfortable and must be changed after having provided care for a service user isolated with any other suspected or known infectious pathogens and when leaving respiratory pathway areas.
It is recommended that Type IIR FRSMs should be well fitting and fit for purpose, covering the mouth and nose in order to prevent venting (exhaled air ‘escaping’ at the sides of the mask). A poster provides some suggested ways to wear facemasks to help improve fit.
Health and care staff moving between different settings, wards and departments to provide care/consultations or undertake service user transfers (e.g. portering and theatre staff) throughout the course of their working day must ensure they first clarify with the person in charge or named health and care worker what pathway the service user they are attending to is on and what PPE is required.
Table 5 PPE worn for SICPs and TBPs (see table 6 for AGP PPE)
PPE item |
Non Respiratory pathway (SICPs)* |
Respiratory pathway (TBPs) |
|---|---|---|
Gloves |
Risk assessment - wear if contact with blood and body fluid (BBF) is anticipated. Single-use |
Worn for all direct care delivery. Single use. |
| Apron or gown |
Risk assessment - wear apron if direct contact with service user, their environment or BBF is anticipated. (Gown if extensive splashing anticipated) Single use |
Apron to be worn for all direct care delivery (Gown if extensive splashing anticipated) Single-use |
Face mask (FRSM)/FFP3 respirator |
Always within 2 metres of a service user- Type IIR FRSM (Wearing a Type IIR FRSM as part of SICPs would normally only be worn when splash/spray is anticipated. Use of FRSM for all service user direct care and exists as an ongoing COVID-19 pandemic measure) Single use or Sessional use |
Always within 2 metres of a service user - Type IIR FRSM FFP3 respirator required when caring for service user with a known or suspected pathogen transmitted by the airborne route e.g. pulmonary TB Single use or Sessional use |
|
Eye & face protection |
Risk assessment - wear if splashing or spraying with BBF including coughing/sneezing anticipated. Single-use or reusable following decontamination. |
Worn for all direct care delivery provided to service users with respiratory symptoms Single-use, sessional or reusable following decontamination. |
*Ensure that PPE is worn appropriately for TBPs as per NIPCM/ on the non-respiratory pathway if caring for service users with any other known or suspected infectious pathogen requiring TBPs.
5.15.5 Access to PPE
NHS staff should continue to obtain PPE through their health board procurement contacts, who will raise their needs via an automated procurement portal to NHS National Services Scotland (NHS NSS). This automated internal procurement system has been specifically developed to deal with increased demand, give real time visibility to Health Boards for ordered stock, as well as enabling quick turnaround for delivery.
Those providing services within social care settings (including personal assistants and unpaid carers) who have an urgent need to access PPE, can contact the PPE support centre on 0300 303 3020 or their local HSCP PPE hub.
Please note that hubs are to be used only in cases where there is an urgent supply shortage after “business as usual” routes have been exhausted.
The contact details below will direct social care providers to the NHS National Services Scotland Social Care PPE Support Centre, and the team there will point you towards your local Hub.
Email: support@socialcare-nhs.info
Phone: 0300 303 3020.
The helpline is open (8am - 8pm) 7 days a week.
Further information can be found at: Coronavirus (COVID-19): PPE access for social care providers and unpaid carers.
5.15.6 Aerosol Generating Procedures (AGPs)
An AGP is a medical procedure that can result in the release of airborne particles from the respiratory tract when treating someone who is suspected or known to be suffering from an infectious agent transmitted wholly or partly by the airborne or droplet route. It is also possible for asymptomatic and pre-symptomatic carriers of COVID-19 to transmit COVID-19 during AGPs.
A full list of AGPs can be found in Appendix 17 of the NIPCM.
5.15.7 Determining the IPC precautions required for AGPs.
Prior to undertaking an AGP, clinical teams must first check that the patient has not developed any new onset respiratory symptoms. Airborne precautions are required for all patients undergoing an AGP on the respiratory pathway. Airborne precautions are also required for patients on the non-respiratory pathway unless there is evidence of a negative COVID-19 test in the 48 hours preceding the AGP in which case droplet precautions may be applied. This recognises the risk of asymptomatic and pre-symptomatic carriage of COVID-19 and the resulting risk of aerosolising the virus during the AGP. Ideally, the negative test should be as close to the point of undertaking the AGP as possible but ideally no more than 48 hours before.
Testing methods used to de-escalate from airborne to droplet precautions during an AGP must be agreed by local board laboratory services in conjunction with Infection Prevention and Control Teams. LFDs must not be used to determine IPC precautions required for AGPs.
Table 6: Precautions required for AGPs
| Service user pathway |
Test result/
|
Precautions required |
Post AGP fallow time required |
Post AGP management of service users. |
|---|---|---|---|---|
|
Respiratory pathway |
Not applicable |
Airborne precautions |
Yes |
Continue on respiratory pathway in line with guidance |
|
Non-respiratory pathway |
COVID-19 negative in previous 48 hours |
Droplet Precautions |
No |
Continue on non -respiratory pathway in line with guidance |
| Non Respiratory pathway |
COVID-19 positive in previous 48 hours*1 |
Airborne precautions |
Yes |
Clinical assessment and discussion with IPCT required to determine suitable pathway for the patient*2. Primary care/OPDs – should consider deferring treatment |
|
Non Respiratory pathway |
Last COVID-19 test result more than 48 hours prior to AGP being undertaken |
Undertake PCR test. Airborne precautions if necessary to proceed to AGP before awaiting test result |
Yes |
Continue on non - respiratory pathway in line with guidance |
|
Non Respiratory pathway |
Unable to obtain COVID-19 test or service user refusal to take a COVID-19 test |
Airborne precautions |
Yes |
Continue on non -respiratory pathway in line with guidance |
*1 Consider immediate management of patient including suitable patient placement based on a positive result. Liaise with clinical team and IPCT to determine appropriate IPC control measures.
*2 If a patient has been tested within 90 days of a previous positive COVID-19 test, clinical teams should consider if the patient may have developed a new respiratory virus or whether the test has detected old inactive virus.
Precautions needed for AGP's Algorithm


Dental Settings
It is recognised that dental practices are unable to utilise PCR testing prior to undertaking AGPs and therefore all patients requiring an AGP regardless of whether they are on the respiratory or non-respiratory pathway will require application of airborne precautions and resulting post AGP fallow times.
5.15.8 PPE for AGPs
The required PPE when undertaking AGPs is listed in table 7.
**Work is currently underway by the UK Re-useable Decontamination Group examining the suitability of respirators, including powered respirators, for decontamination. This literature review will be updated to incorporate recommendations from this group when available. In the interim, ARHAI Scotland are unable to provide assurances on the efficacy of respirator decontamination methods and the use of re-useable respirators is not recommended.
Table 7: PPE for AGPs
PPE Item |
Non Respiratory pathway (SICPs) where there is evidence of a negative COVID-19 test within the preceding 48 hours |
Respiratory pathway (TBPs) and Non Respiratory pathway where there is no evidence of a COVID-19 test within the preceding 48 hours |
|---|---|---|
Gloves |
Single-use |
Single use |
Apron or gown |
Single-use Risk assess – use fluid resistant gown if excessive splashing/spraying anticipated otherwise apron is sufficient |
Single-use fluid resistant gown |
Face mask (FRSM) or Respirator |
Type IIR FRSM* Single or Sessional use |
FFP3 mask or powered respirator hood Single or Sessional use |
|
Eye & face protection |
Single use or reusable following decontamination |
Single-use, sessional or reusable following decontamination |
*Where staff have concerns about potential COVID-19 exposure to themselves during this ongoing COVID-19 pandemic, they may choose to wear an FFP3 respirator rather than an FRSM when performing an AGP on any patient provided they are fit tested. This is a personal PPE risk assessment.
5.15.9 Post AGP Fallow Times
Time is required after AGPs undertaken with airborne precautions are performed to allow the actual/potential infectious aerosols still circulating to be removed/diluted. This is referred to as the post AGP fallow time (PAGPFT) and is a function of the room ventilation air change rate. The PAGPFTs can be found in appendix 17 of the NICPM.
Dental settings - AGPs
Staff within dental settings should refer to the ‘Mitigation of AGPs in dentistry; A Rapid Review’ which details fallow times specific to this setting and the mitigations used. The methodology work was undertaken by SDCEP and Cochrane oral Health. Post AGP down time (fallow time) is not considered necessary for successive appointments between members of the same household within dental settings; to minimise aerosol spread dentists should use mitigating measures such as high volume suction/rubber dam. It is essential that staff change their PPE and adhere to SICPs between family members.Treatment rooms in dental practices should be aiming for a minimum of 10ACH.
Draft 5.16 Safe Management of Care Equipment
See NIPCM for routine safe management of care equipment as per SICPs.
 Care Home Settings
Care Home Settings
Care homes should refer to the NIPCM for older people and adult care homes for more general information on safe management of care equipment in this setting as per SICPs.
Care equipment used for service users on the respiratory pathway may become contaminated with infectious transmissible pathogens and must be cleaned as per table 8.
Table 8: Equipment cleaning determined by SICPs/TBPs
Pathway |
Product |
|---|---|
|
Routine care areas (non-respiratory pathway) – cleaning as per SICPs |
General purpose detergent for routine cleaning. |
|
Respiratory pathway -cleaning as per TBPs |
Combined detergent/disinfectant solution at a dilution of 1000 ppm av chlorine or general purpose neutral detergent in a solution of warm water followed by a disinfectant solution of 1000ppm av chlorine for routine cleaning. |
See Appendix 7 of the NIPCM for cleaning of equipment contaminated with blood or body fluids (including saliva) or if it has been used on a patient with any other known or suspected infectious pathogen.
 Primary Care and Community Health and Social Care settings
Primary Care and Community Health and Social Care settings
Equipment cleaning for care at home services
Re-useable care equipment used on the respiratory pathway in the community health and care settings such as stethoscopes, syringe drivers and pumps must be decontaminated prior to removal from the service user’s home. Where this is not possible, they should be bagged and transported back to base for decontamination.
Draft 5.17 Safe Management of the care environment
See NIPCM for routine safe management of care environment as per SICPs.
 Care Home Settings
Care Home Settings
Care homes should refer to the Care Home IPCM for older people and adult care homes for more general information on safe management of the care environment in this setting as per SICPs.
Environmental cleaning in the respiratory pathway should be undertaken as per table 8. A minimum of 4 hours should have elapsed between the first daily clean and the second daily clean. Where a room has not been occupied by any staff or service user since the first daily clean was undertaken, a second daily clean is not required.
Table 9 - Environmental cleaning determined by SICPs/TBPs
Pathway |
Frequency |
Product |
|---|---|---|
|
Routine care areas (non-respiratory pathway) – cleaning as per SICPs |
At least daily as per NHS Scotland National Cleaning Services Specification.
|
General purpose detergent*
|
|
Respiratory pathway - cleaning as per TBPs (incl post AGP for service users requiring airborne precautions for AGPs) |
At least twice daily 1st clean - Full clean (domestic services) 2nd clean - * Touch Surfaces within clinical and care delivery areas |
Combined detergent/disinfectant solution at a dilution of 1000 ppm av chlorine or general purpose neutral detergent in a solution of warm water followed by a disinfectant solution of 1000ppm av chlorine.
|
*Cleaning in routine care areas should be carried out with chlorine based detergent for rooms where the service user is known to have any other known or suspected infectious agent.
* Touch surfaces as a minimum should include door handles/push pads, taps, bed heads/bed ends, cot sides, light switches, lift buttons. Clinical and care delivery areas should include the service user’s bedroom and treatment areas and staff rest areas.
Any areas contaminated with BBF (including saliva) in any clinical/care area require to be cleaned as per Appendix 9 of the NIPCM.
In settings such as outpatient departments, GP practices, dental practices, where there are multiple service users undergoing a consultation each day, cleaning should be undertaken between service users in addition to the environmental cleaning described above using the appropriate cleaning product depending on the pathway the service user is on. Ensure that any surfaces touched by the service user are cleaned e.g. chair, treatment bed and where the service user is symptomatic of a respiratory virus, cleaning should include items in the immediate environment which may have become contaminated.
Draft 5.18 Safe management of linen
All linen should be handled routinely as per section 1.7 of SICPs – Safe Management of Linen
 Care Home Settings
Care Home Settings
Care homes should refer to the Care Home IPCM for older people and adult care homes for more general information on safe management of linen in this setting as per SICPs.
Linen used on service users who are on the respiratory pathway should be treated as infectious.
Routinely on the respiratory pathway, provided curtains around examination bays have no visible contamination and are kept tied back when not in use, they may remain in situ situ between patients however regular curtain change regimes should be in place. Curtains should also be cleaned as part of terminal cleaning following discontinuation of TBPs and following discharge of a patient from inpatient settings where transmission based precautions were in place at the time of discharge. When changed, curtains should be treated as infectious linen.
 Primary Care and Community Health and Social Care settings
Primary Care and Community Health and Social Care settings
Safe Management of Laundry
Community Health and Care Settings with their own in-house laundries may also refer to National Guidance for Safe Management of Linen in NHSScotland for more information.
See staff uniforms.
Draft 5.19 Safe management Blood and Body Fluid spillages
All BBF spillages should be managed as per section 1.8 of SICPs – Safe management of Blood and Body Fluid Spillages and Appendix 9.
 Care Home Settings
Care Home Settings
Care homes should refer to the Care Home IPCM for older people and adult care homes for general information on safe management of Blood and Body Fluid spillages.
Waste generated during the management of BBF spillages should be disposed of as waste section.
Draft 5.20 Safe management of waste
Waste should be handled in accordance with Section 1.9 of SICPs. Any items contaminated with BBF (including saliva) for any patient regardless of infectious status should be disposed of as clinical waste.
 Care Home Settings
Care Home Settings
Care homes should refer to the Care Home IPCM for older people and adult care homes for more general information on safe management of waste in this setting.
Waste generated from patients/individuals who are on the respiratory pathway or where there is a confirmed outbreak, should be disposed of as clinical waste where clinical waste contracts are in place.
 Primary Care and Community Health and Social Care settings
Primary Care and Community Health and Social Care settings
If the community health and care setting does not have a clinical waste contract, or for care at home, ensure all waste items (e.g. used tissues and disposable cleaning cloths) that have been in contact with service users who are known or suspected to have COVID-19 are disposed of securely within disposable bags. When full, the plastic bag should then be placed in a second bin bag and tied. These bags should be stored in a secure location for 72 hours before being put out for collection.
Draft 5.21 Occupational Safety
Employers have a duty of care to their staff. This is enshrined in health and safety legislation as is the requirement to undertake a risk assessment and then to mitigate any risks as low as reasonably practicable.
Section 1.10 of the NIPCM details occupational safety as per SICPs.
Care Home Settings
Care homes should refer to the Care Home IPCM for older people and adult care homes for more general information on occupational safety in this setting.
PPE is provided for occupational safety and should be worn as per Tables 7 and 8.
Staff testing negative for SARS-CoV-2 by PCR who remain symptomatic of another respiratory virus should consider the risk to service users particularly if they are immunosuppressed or otherwise medically vulnerable before returning to work. Once medically fit to return to work, if staff are in doubt about any risk they may pose to service users or colleagues, this should be discussed with their line manager in the first instance.
Decisions to deploy any staff members into areas of higher infection risk must take into account many factors. These include the nature of the biologic agent, the general risks, and the specific risks to each individual member of staff. The individual risk assessment may need to take account of age, gender, underlying health conditions, race and vaccine status amongst other factors. Occupational health expertise should be sought regarding both the overall process and for individuals deemed at significantly higher risk of either acquiring the infection or of an adverse outcome should they acquire infection.
Boards must have systems for risk assessment and mitigation with clearly defined responsibilities, routes to obtain advice from health and safety, occupational health, and other specialist advisers where required.
Occupational risk assessment guidance specific to COVID-19 is available. Further information for at risk or pregnant healthcare workers can be found in Guidance for Staff and Managers on Coronavirus
5.21.1 Vehicle sharing for all staff during the ongoing COVID-19 pandemic
Wherever possible, vehicle sharing should be avoided with anyone outside of household or support bubbles. This is an ongoing COVID-19 pandemic measure and exists because the close proximity of individuals sharing the small space within the vehicle increases the risk of transmission of respiratory infections including COVID-19. All options for travelling separately should be explored and considered such as;
- Staff travelling separately in their own vehicles
- Geographical distribution of visits – can these be carried out on foot or by bike?
- Use of public transport where social distancing can be achieved via use of larger capacity vehicles
However, it is recognised that there are occasions where vehicle sharing is unavoidable such as:
- Staff who carry out community visits.
- Staff who are commuting with students as part of supported learning/mentorship.
- Staff working in emergency response vehicles (not patient vehicles).
- Staff living in areas where public transport is limited and vehicle sharing is the only means of commuting to and from the workplace.
Where vehicle sharing cannot be avoided, staff should adhere with the guidance below to reduce any risk of cross transmission:
- Staff (and students) must not travel to work/vehicle share if they have symptoms compatible with a diagnosis of COVID-19.
- Ideally, no more than 2 people should travel in a vehicle at any one time (with the exception of some response vehicles and home care visits which may require more than 2 people - a risk assessment should be undertaken locally).
- Use the biggest vehicle available for sharing purposes.
- Vehicle sharing should be arranged in such a way that staff share the journey with the same person each time to minimise the opportunity for exposure. Rotas should be planned in advance to take account of the same staff commuting together/vehicle sharing as far as possible.
- The vehicle must be cleaned regularly (at least daily) and particular attention should be paid to high risk touch points such as door handles, electronic buttons and seat belts. General purpose detergent is sufficient (detergent wipes may be used) unless a symptomatic or confirmed case of COVID-19 has been in the vehicle in which case a disinfectant should be used.
- Occupants should sit as far apart as possible, ideally the passenger should sit diagonally opposite the driver.
- Windows in the vehicle must be opened as far as possible taking account of weather conditions to maximise the ventilation in the space.
- Occupants in the vehicle, including the driver, should wear a Type IIR FRSM provided it does not compromise driver safety in any way.
- Occupants should perform hand hygiene using ABHR before entering the vehicle and again on leaving the vehicle. If hands are visibly soiled, use ABHR on leaving the vehicle and wash hands at the first available opportunity.
- Occupants should avoid eating in the vehicle.
- Passengers in the vehicle should minimise any surfaces touched, it is not necessary for vehicle occupants to wear aprons or gloves.
- Keep the volume of any music/radio being played to a minimum to prevent the need to raise voices in the vehicle.
Draft 5.22 Staff Uniforms
It is safe to launder uniforms at home. If the uniform is changed before leaving work, then transport this home in a disposable plastic bag or a launderable bag. If your role requires you to wear a uniform to and from work, then change as soon as possible when returning home.
Uniforms should be laundered daily, and:
- separately from other household linen;
- in a load not more than half the machine capacity;
- at the maximum temperature the fabric can tolerate, then ironed or tumble dried.
Scottish Government uniform, dress code and laundering policy is available.
Contaminated uniforms and surgical scrubs should be laundered in hospital (dedicated laundry) facilities as per local policies.
Draft 5.23 - Caring for someone who has died
For deceased who were on the respiratory pathway at the time of death, the IPC measures described in this document continue to apply whilst the deceased remains in the health and care environment. This is due to the ongoing risk of infectious transmission via contact although the risk is usually lower than for living service users. Where the deceased was known or suspected to have been infected with COVID-19, there is no requirement for a body bag, and viewing, hygienic preparations, post-mortem and embalming are all permitted. Body bags may be used for other practical reasons such as maintaining dignity or preventing leakage of body fluids. See IPC during care of the deceased within the NIPCM for more information.
 Care Home Settings
Care Home Settings
Care homes should refer to the Care Home IPCM for older people and adult care homes for more general information on care of the deceased in this setting.
For further information see the Scottish Government Coronavirus (COVID-19): guidance for funeral directors on managing infection risks.
Draft 5.24 - Visiting to health and care settings
Scottish government have guidance available for visiting which can be found at the following links;
Hospital visiting - https://www.gov.scot/publications/coronavirus-covid-19-hospital-visiting-guidance/
Care home visiting - https://www.gov.scot/publications/coronavirus-covid-19-adult-care-homes-visiting-guidance/
All visitors must be informed on arrival at any health and care facility of IPC measures and adhere to these at all times. Visitors should wear face coverings in line with current Scottish Government guidance and must not attend with COVID-19 symptoms or before a period of self-isolation has ended, whether identified as a case of COVID-19 or as a contact. Visiting may be suspended on the advice of the local IPCT/HPT. Consider alternative measures of communication including telephone or video call where visiting is not possible.
Visitors must:
- Not visit if they have suspected or confirmed COVID-19 or if they have been advised to self-isolate for any reason unless prior agreement with clinical teams during specific circumstances;
- Not visit if they have symptoms of another viral infection e.g. respiratory symptoms, GI symptoms unless prior agreement with clinical teams during specific circumstances.
- Wear a face covering on entering the facility;
- Be provided with appropriate PPE (see table 7);
- Perform hand hygiene at the appropriate times;
- on entry to the facility
- prior to putting on PPE
- after removing PPE
- Observe physical distancing; Visitors may have touch contact with loved ones (hug/kiss) however are reminded that maintaining 1 metre or more distancing out with direct touch contact wherever possible will help reduce the risk of transmission of COVID-19 and other respiratory pathogens to them, their loved one and others in the health and care setting.
- Not move around the facility and should stay at the bed or chairside of the individual they are visiting;
- Not visit other service users in the facility;
- Not touch their face or face covering/mask once in place;
- Not eat whilst visiting;
- Avoid sharing mobile phone devices with the individual unnecessarily – if mobile devices are shared to enable communications with other friends and family members, the phone should be cleaned between uses using manufacturer’s instructions.
Table 10 – Visitor PPE
Pathway |
Gloves |
Apron |
Face covering/mask |
Eye/Face Protection |
|---|---|---|---|---|
|
Routine care areas (SICPs) |
Not required*1 |
Not required*2 |
Face covering or provide with Type IIR FRSM if visitor arrives without a face covering |
Not required*3 |
|
Respiratory pathway (TBPs) |
Not required*1 |
Not required*2 |
Type IIR FRSM |
If within 2 metres of service user with respiratory symptoms |
*1 unless providing direct care which may expose the visitor to blood and/or body fluids i.e. toileting.
*2 unless providing care resulting in direct contact with the service user, their environment or blood and/or body fluid exposure i.e. toileting, bed bath.
*3 Unless providing direct care and splashing/spraying is anticipated.
Draft 5.25 - Resources
PPE posters
PPE for delivery of COVID-19 vaccination (staff)
PPE for attending for your COVID-19 vaccination (public)
Wearing a facemask poster (staff)
Draft Appendix 1 Respiratory Algorithm for use across all health and care settings

A printable version of this algorithm is available.
{kind=link}
Content
- Draft 5.1 Introduction
- Draft 5.2 Organisational Preparedness
- Draft 5.3 Hierarchy of controls
- Draft 5.4 Physical distancing
- Draft 5.5 General Infection Prevention and Control Information
- Draft 5.6 Case definitions and symptomology
- Draft 5.7 Respiratory screening assessment to determine transmission risk
- Draft 5.8 Placement and management of a service user with respiratory symptoms
- Draft 5.9 Respiratory testing for service users
- Draft 5.10 Respiratory Screening for Healthcare Workers (HCW)
- Draft 5.11 Duration of Transmission Based Precautions for respiratory pathogens (excl COVID-19)
- Draft 5.12 - Duration of transmission based precautions for COVID-19
- Draft 5.13 - Hand Hygiene
- Draft 5.14 - Respiratory etiquette
- Draft 5.15 - Personal Protective Equipment (PPE)
- Draft 5.16 Safe Management of Care Equipment
- Draft 5.17 Safe Management of the care environment
- Draft 5.18 Safe management of linen
- Draft 5.19 Safe management of Blood and Body Fluid spillages
- Draft 5.20 Safe management of waste
- Draft 5.21 Occupational Safety
- Draft 5.22 Staff Uniforms
- Draft 5.23 - Caring for someone who has died
- Draft 5.24 - Visiting to health and care settings
- Draft 5.25 - Resources
- Draft Appendix 1 Respiratory Algorithm for use across all health and care settings